

Nail Signs of Premature Aging
 Faramarz Rafie MD, DBA / Vancoderm Academy and College (VDA) / Vancoderm Clinic (VDCMed)
Faramarz Rafie MD, DBA / Vancoderm Academy and College (VDA) / Vancoderm Clinic (VDCMed)
Aging is traditionally evaluated through cutaneous and facial biomarkers; however, the nail unit—comprising the nail matrix, nail bed, nail plate, and periungual tissues—serves as a clinically informative structure for assessing both physiological and pathological aging processes. From a dermatological and medical aesthetics perspective, alterations in nail morphology, growth kinetics, and keratin integrity provide objective indicators of chronological aging as well as premature (extrinsic or accelerated) aging driven by environmental, systemic, and lifestyle-related factors.
At the cellular level, age-related changes in the nail apparatus are primarily mediated by reduced proliferative capacity of matrix keratinocytes, diminished vascular perfusion, and cumulative oxidative stress. These mechanisms result in measurable changes such as decreased linear nail growth rate, altered keratinization, and compromised intercellular cohesion within the nail plate. In premature aging, these processes are exacerbated by exogenous insults—including ultraviolet radiation, chemical exposure, and microtrauma—as well as endogenous contributors such as micronutrient deficiencies, endocrine imbalance, and impaired microcirculation.
Clinically, detailed nail examination allows practitioners to distinguish between intrinsic senescence and accelerated degeneration. Parameters such as longitudinal ridging (onychorrhexis), lamellar splitting (onychoschizia), chromatic alterations, and periungual tissue atrophy are not merely cosmetic concerns but reflect underlying biochemical and structural changes. Accordingly, the nail unit should be regarded as a diagnostic extension of the integumentary system, offering valuable insight into both localized aging phenomena and systemic health status.
 Understanding Nail Aging: Chronological vs. Premature (Advanced Medical Perspective)
Understanding Nail Aging: Chronological vs. Premature (Advanced Medical Perspective)
Chronological nail aging represents an intrinsic, genetically programmed, time-dependent process affecting the entire nail unit, particularly the nail matrix and its keratinocyte population. With advancing age, there is a progressive decline in matrix keratinocyte proliferative activity, associated with reduced mitotic index and altered expression of structural keratins (notably hard keratins K31–K40). This results in a measurable decrease in linear nail growth rate (approximately 0.5–1.2 mm/week in younger adults, declining with age).
At the molecular level, intrinsic aging is driven by:
- Cellular senescence and telomere shortening
- Reduced ATP production and mitochondrial efficiency
- Accumulation of reactive oxygen species (ROS) leading to oxidative damage
- Decline in dermal microvascular perfusion, impacting oxygen and nutrient delivery to the matrix
- Altered intercellular lipid composition, affecting nail plate cohesion and hydration
Clinically, chronological aging manifests as:
- Fine longitudinal ridging (onychorrhexis) due to uneven matrix activity
- Mild opacity and decreased translucency of the nail plate
- Slight increase in brittleness due to reduced water-binding capacity
- Gradual thickening or thinning depending on individual and vascular factors
These changes are typically symmetric, slowly progressive, and consistent with the patient’s age.
In contrast, premature nail aging (also referred to as extrinsic or accelerated nail aging) is characterized by pathologically enhanced degenerative changes occurring earlier than expected, often with greater clinical severity. This form of aging reflects the cumulative impact of exogenous insults and endogenous dysregulation, which amplify the biological pathways seen in intrinsic aging.
Key pathogenic mechanisms include:
- Chronic oxidative stress exceeding endogenous antioxidant capacity
- Glycation of nail matrix proteins, impairing keratin structure and resilience
- Disruption of barrier function due to repeated chemical and solvent exposure
- Microinflammatory processes within the matrix and periungual tissues
- Compromised peripheral microcirculation, often linked to smoking or systemic disease
- Nutritional insufficiencies affecting keratin synthesis (e.g., biotin, iron, sulfur-containing amino acids)
Clinically, premature nail aging presents with:
- Pronounced onychorrhexis and onychoschizia (lamellar splitting)
- Surface roughness and irregularity beyond age-expected norms
- Dyschromia (yellowing, dullness, or uneven pigmentation)
- Increased fragility and susceptibility to mechanical trauma
- Periungual atrophy, including cuticle loss and xerosis
- Occasionally subungual hyperkeratosis or altered adhesion between nail plate and bed
Unlike chronological aging, these changes may be asymmetric, rapidly progressive, and frequently associated with identifiable risk factors such as occupational exposure, cosmetic practices, or underlying systemic pathology.
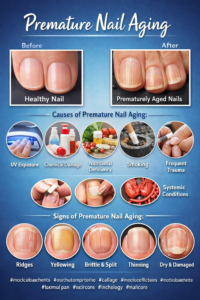
Etiology of Premature Nail Aging
Premature nail aging is a multifactorial, pathophysiological process involving cumulative damage to the nail matrix, nail bed, and nail plate. It reflects the interaction between extrinsic environmental insults and intrinsic systemic dysregulation, ultimately leading to impaired keratinization, structural fragility, and altered nail growth dynamics.
Chronic ultraviolet (UV) exposure and photoaging
The nail unit is susceptible to photoaging, particularly with repeated sun exposure or use of UV-based nail devices. Ultraviolet radiation, especially UVA, induces reactive oxygen species within matrix keratinocytes. This results in oxidative damage to keratin proteins, lipids, and cellular DNA, promoting premature cellular senescence and reduced proliferative capacity. Over time, this contributes to yellow discoloration, loss of translucency, and increased brittleness. In addition, degradation of intercellular lipids compromises nail plate cohesion and hydration.
Repeated chemical exposure
Chronic exposure to chemical agents, common in both occupational environments and cosmetic nail procedures, significantly alters nail integrity. Organic solvents such as acetone and ethyl acetate dissolve intercellular lipids, increasing transepidermal water loss from the nail plate. Detergents and alkaline substances disrupt keratin cross-linking, weakening the structural framework. Clinically, this manifests as lamellar splitting (onychoschizia), surface roughness, and increased fragility. Persistent exposure may also induce low-grade inflammation in the periungual tissues and matrix, further impairing nail formation.
Nutritional deficiencies
Proper nail formation depends on adequate intake of micronutrients and amino acids essential for keratin synthesis and cellular metabolism. Biotin deficiency disrupts keratin infrastructure, leading to brittle nails. Iron deficiency reduces oxygen delivery to the nail matrix and may result in structural deformities such as koilonychia. Zinc deficiency interferes with protein synthesis and cellular repair, while insufficient protein intake limits sulfur-containing amino acids necessary for disulfide bond formation in keratin. These deficiencies collectively result in reduced matrix activity, abnormal keratinization, and decreased nail plate resilience.
Systemic conditions
Systemic disorders contribute to premature nail aging through vascular, metabolic, and hormonal pathways. Thyroid dysfunction alters nail physiology, with hypothyroidism causing slow growth and brittleness, and hyperthyroidism leading to soft, thin nails with potential onycholysis. Peripheral vascular insufficiency reduces oxygen and nutrient delivery to the nail matrix, resulting in atrophic changes and impaired regeneration. Chronic conditions such as anemia, renal disease, and hepatic dysfunction further compromise cellular turnover and keratin production, often presenting as diffuse nail dystrophy.
Smoking and microcirculatory impairment
Smoking exerts significant effects on nail aging through vascular and biochemical mechanisms. Nicotine induces vasoconstriction, reducing blood flow to the nail matrix, while carbon monoxide decreases oxygen delivery. Increased oxidative stress leads to cellular damage and impaired repair processes. Additionally, accumulation of toxins contributes to discoloration and loss of nail luster. The overall effect is diminished matrix function, delayed growth, and compromised structural integrity.
Repetitive mechanical trauma
Mechanical trauma is a common contributor to premature nail aging, particularly in individuals undergoing frequent cosmetic nail procedures. Aggressive manicuring, over-filing, and improper use of nail enhancements disrupt the structural layers of the nail plate and may affect the matrix. Repeated trauma leads to irregular keratin deposition, longitudinal ridging, thinning, and deformity. In chronic cases, matrix injury may result in scarring and persistent nail dystrophy.
Dehydration of the nail plate and matrix
Hydration plays a critical role in maintaining nail flexibility and mechanical strength. The nail plate normally contains a significant water component, which supports its elasticity. Loss of intercellular lipids increases water permeability and evaporation, leading to brittleness, fragility, and splitting. Dehydration also alters the biomechanical properties of the nail, reducing its resistance to mechanical stress. Environmental factors such as low humidity, frequent handwashing, and chemical exposure exacerbate this process and impair keratinocyte differentiation within the matrix.
Clinical Signs of Premature Nail Aging
Practitioners should be vigilant in identifying early indicators, including:
- Longitudinal ridging (onychorrhexis) beyond age-expected norms
- Brittleness and splitting (onychoschizia)
- Thinning or thickening of the nail plate
- Loss of natural luster and increased opacity
- Yellowing or dyschromia
- Slower growth rate inconsistent with patient age
- Subungual hyperkeratosis in some cases
- Periungual dryness and cuticle degeneration
Preventative care remains the most effective strategy in managing premature nail aging:
 VANCODDERM ACADEMY AND COLLEGE
VANCODDERM ACADEMY AND COLLEGE